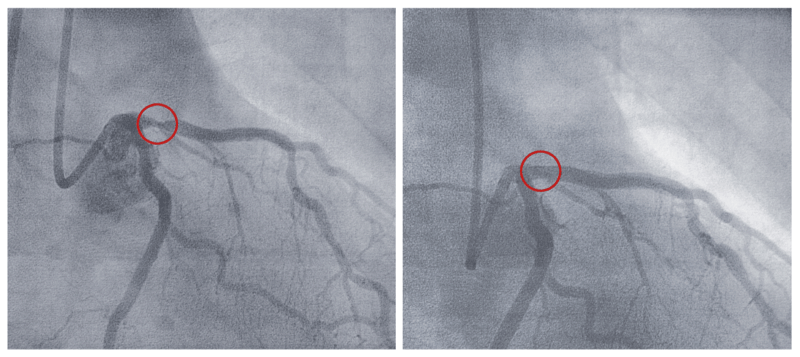
Coronary angioplasty/stenting, also called percutaneous coronary intervention (PCI) or the balloon and stent procedure, is a treatment used to deal with tight narrowings in the coronary arteries that are affecting the blood supply to the heart (the images to the right show a narrowed artery before and after it has been reopened with angioplasty and stenting).
First developed in the 1970s it was originally used in stable “elective” situations to treat angina caused by a narrowing in one coronary artery. These days angioplasty is a highly effective treatment for many patients with a number of narrowings in one or more coronary arteries, and not only in the stable elective situation but also in urgent situations and the emergency treatment of a heart attack, known as primary angioplasty, where it is the treatment of choice.
The technique bears some similarities to coronary angiography, in that it is also performed in the catheter laboratory with very similar equipment, but there are also fundamental differences, the most important being that angiography is an investigative tool, but angioplasty is a treatment.
During the procedure itself, under local anaesthetic a fine flexible tube 2 to 3 mm in diameter is passed up the artery from the wrist, or if necessary, from the groin, to the coronary artery using X-ray guidance.
A very small deflated balloon is then passed over the wire and up to the site of the narrowing. There it is inflated, pushing the atheroma (furring up) into the vessel wall to relieve the obstruction to blood flow. In nearly all patients a stent is inserted at this site to minimise the risk of the artery blocking in the first few weeks and months after the procedure.
A stent is essentially a precision-made tube of mesh, constructed from medical grade stainless steel or other metals and alloys, premounted on a deflated angioplasty balloon, so that when the balloon is inflated the stent expands to form a scaffold to keep the artery open. Nearly all stents used these days are coated with a drug which reduces the risk of regrowth and narrowing in the stent (restenosis). They are known as drug-eluting stents (DES), in contrast with bare metal stents (BMS), which are not coated in antiproliferative drugs. The stent is a permanent device which remains in the artery when the deflated balloon is removed.

In the last decade or so, much research has also been undertaken into bioabsorbable stents, which gradually dissolve over time, leaving behind only the healed natural artery. Results to date have been mixed but this continues to be an area provoking considerable interest and research.
After stent implantation the coronary artery forms a thin layer of cells over the stent struts. Until this is complete the metal struts have the potential to provoke clot formation within the stent, which carries the risk of a heart attack. This is minimised by dual antiplatelet therapy, taking a combination of two blood thinners, aspirin and either clopidogrel, ticagrelor or prasugrel, for a set period of time, determined by the clinical scenario and the type of stent implanted. Bare metal stents may only need this combination therapy for one month if implanted in an elective situation, while drug-eluting stents may require the combination for up to one year and sometimes more. Most patients treated as emergency cases are given this treatment for up to a year, following which most patients can stop one of the drugs. There are also occasions where a patient may be advised to remain on both drugs indefinitely.
In preparation for the procedure the patient must not eat or drink for 4 to 6 hours beforehand; usual medication should be taken with a sip of water, but generally speaking diuretics such as furosemide are omitted on the day. Diabetics are given special advice, particularly those taking metformin or insulin, as are patients on warfarin or other anticoagulants such as dabigatran, apixaban, rivaroxaban and edoxaban.
In elective cases where the procedure has been straightforward the patient will likely go home the same day, or perhaps stay in hospital overnight if the procedure was undertaken later in the day. The patient should avoid strenuous activity in the days following the procedure and should not drive for a week.